Article by: Dr. Gajanan Bhalerao (PT) MPT neuro PT , C/NDT (USA), Aquatic therapy (Kliniken Valens Switzerland)

Physical Therapy is a constantly evolving field. There are many types and methods are adding as adjunct traditional physical therapy. Most of these therapies are performed on the land. There are multiple forces are always acting on our body in any given instant. the forces can be internal or external forces. Our muscles and body mechanics always have work against or with these forces to move. There is always one force acts on everything including our body is the constant force of gravity. Gravity acts on everything all the time. We move against or towards the force of gravity. We try to stabilize our body against the force of gravity. Amount of muscles work and effort depends on what is the body alignment with respect to gravity.
Benefit from Aqua therapy
- Reduce weight bearing on lower limb – helps in partial weight bearing walking gradation


- Assist in stability and balance
- Makes Movement easy and assisted
- Gives resistance to movements,
- Easy to change the grading of resistance
- High intensity training with less fatigue and injury to muscles and ligaments
- Less stress on ligaments in closed chain positions
- Helps in general body relaxation – stress management
- Joint mobilization hip, knee, ankle, shoulder & elbow with less pain even with high intensity mobilization
- Improving range of motion
- Spinal joint mobilization
- Muscle relaxation
- Non weight bearing walking – deep water walking with floats
- Strength training
- Endurance training
- Agility & plyometrics training
- Balance training
- Reduce tone/spasticity /rigidity/ tightness
- Graded loading on labrum/ capsule and ligaments of joints
- Coordination training
Whom to contact for aquatic therapy?
Ans -Dr. Gajanan Bhalerao, 9822623701. schoolneurorehab@gmail.com
GB school of neuro rehab and aquatic therapy, Bungalow no 1. Gajanan Housing society Model colony Shivajinagar Pune 16. Direction and Maps
WHAT IS AQUATIC THERAPY?
There are multiple methods are developed to reduce the effect of gravity and using buoyancy.




- Body weight supported treadmill training

")



- Robotic locomat
")
")
")

- Space walk training simulator

- Aqua treadmill
")
")
")
")
")
")
")
")
- Aqua gym
")
")
")
")
")
")
Aqua cycling
")
")
")
All these method of training have advantage and disadvantages.
- Most of these are targeted at only walking training (alter G, body weight supported treadmill training, aqua treadmill), cycling (aqua cycling) and strengthening ( aqua gym) individual muscles.
- Body weight supported treadmill training is not very comfortable for patient (harness and un- weighing). it requires lots of effort by therapist to put legs forward during walking.

- Aqua treadmill : we can do limited exercises of walking forward, backward, sideways or running only.
There is need of therapy where there is more flexibility of selection of therapeutic exercises and activities. So Aquatic therapy play a major role is in this.
What is aquatic therapy?
Aquatic therapy refers to treatments and exercises performed in water for relaxation, fitness, physical rehabilitation, and other therapeutic benefit. Typically a qualified aquatic therapist gives constant attendance to a person receiving treatment in a heated therapy pool. Aquatic therapy techniques include Ai Chi, Aqua Running, Bad Ragaz Ring Method, Burdenko Method, Halliwick, Watsu, and other aquatic bodywork forms. Therapeutic applications include neurological disorders, spine pain, musculoskeletal pain, postoperative orthopedic rehabilitation, pediatric disabilities, and pressure ulcers.
Aquatic therapy refers to water-based treatments or exercises of therapeutic intent, in particular for relaxation, fitness, andphysical rehabilitation. Treatments and exercises are performed while floating, partially submerged, or fully submerged in water. Many aquatic therapy procedures require constant attendance by a trained therapist, and are performed in a specialized temperature-controlled pool. Rehabilitation commonly focuses on improving the physical function associated with illness, injury, or disability.[1][2]
Aquatic therapy encompasses a broad set of approaches and techniques, including aquatic exercise, physical therapy,aquatic bodywork, and other movement-based therapy in water (hydrokinesiotherapy). Treatment may be passive, involving a therapist or giver and a patient or receiver, or active, involving self-generated body positions, movement, or exercise. Examples include Halliwick Aquatic Therapy, Bad Ragaz Ring Method, Watsu, and Ai chi.[1]
For orthopedic rehabilitation, aquatic therapy is considered to be synonymous with therapeutic aquatic exercise, aqua therapy, aquatic rehabilitation, water therapy, and pool therapy. Aquatic therapy can support restoration of function for many areas of orthopedics, including sports medicine, work conditioning, joint arthroplasty, and back rehabilitation programs. A strong aquatic component is especially beneficial for therapy programs where limited or non-weight bearing is desirable and where normal functioning is limited by inflammation, pain, guarding, muscle spasm, and limited range of motion (ROM). Water provides a controllable environment for reeducation of weak muscles and skill development for neurological and neuromuscular impairment, acute orthopedic or neuromuscular injury, rheumatological disease, or recovery from recent surgery.[3]:1
Various properties of water contribute to therapeutic effects, including the ability to use water for resistance in place of gravity or weights; thermal stability that permits maintenance of near-constant temperature; hydrostatic pressure that supports and stabilizes, and that influences heart and lung function; buoyancy that permits floatation and reduces the effects of gravity; and turbulence and wave propagation that allow gentle manipulation and movement.[4]
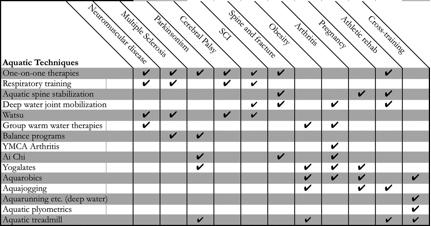
Techniques
Techniques for aquatic therapy include the following:
- Halliwick Concept: The Halliwick Concept, originally developed by fluid mechanics engineer James McMillan in the late 1940s and 1950s at the Halliwick School for Girls with Disabilities in London, focuses on biophysical principles of motor control in water, in particular developing sense of balance (equilibrioception) and core stability. The Halliwick Ten-Point-Program implements the concept in a progressive program of mental adjustment, disengagement, and development of motor control, with an emphasis on rotational control, and applies the program to teach physically disabled people balance control, swimming, and independence.
")
")
")
- Water Specific Therapy, WST: Halliwick Aquatic Therapy (also known as Water Specific Therapy, WST), implements the concept in patient-specific aquatic therapy. This concept is very good for rehabilitation of neurological and orthopedic impairment. This is tailer made approach for individual needs and problems. In this you can on the motor control as whole body & its movements in all direction and individual motor muscle control. You can do task specific training i.e. sit to stand, balance in walking, one leg stance, walking and balance again resistance of water, coordination exercises, core strengthening in task, postural control and motor control in various task.
")
")
")
- Bad Ragaz Ring Method: The Bad Ragaz Ring Method (BRRM) focuses on rehabilitation of neuromuscular function using patterns of therapist-assisted exercise performed while the patient lies horizontal in water, with support provided by rings or floats around the neck, arms, pelvis, and knees. BRRM is an aquatic version of Proprioceptive Neuromuscular Facilitation (PNF) developed by physiotherapists at Bad Ragaz, Switzerland, as a synthesis of aquatic exercises designed by a German physician in the 1930s and land-based PNF developed by American physiotherapists in the 1950s and 1960s.
- https://youtu.be/A0-DGEP4F1U
")
")
")
")
")
")
")
")
")
- Ai Chi: Ai Chi, developed in 1993 by Jun Konno, uses diaphragmatic breathing and active progressive resistance training in water to relax and strengthen the body, based on elements of qigong and Tai chi chuan.
")
")
")
")
")
")
")
- Aqua running: Aqua running (Deep Water Running or Aquajogging) is a form of cardiovascular conditioning, involving running or jogging in water, useful for injured athletes and those who desire a low-impact aerobic workout. Aqua running is performed in deep water using a floatation device (vest or belt) to support the head above water.

")
")
")
")
")

")
")
- Watsu: Watsu is a form of aquatic bodywork, originally developed in the early 1980s by Harold Dull at Harbin Hot Springs, California, in which an aquatic therapist continuously supports and guides the person receiving treatment through a series of flowing movements and stretches that induce deep relaxation and provide therapeutic benefit. In the late 1980s and early 1990s physiotherapists began to use Watsu for a wide range of orthopedic and neurologic conditions, and to adapt the techniques for use with injury and disability.
")
")
")
")
")
")
")
")
")
")
")
")
Healing Dance
Aqua aerobics:
Top 6 reasons to use aqua aerobics for exercise:
1)Heart health. heart rate will be about 13 percent more slower – about 17 fewer heart beats a minute.
2)The enjoyment: If a workout is fun, I’m more likely to keep doing it.
3)The variety.
4)Stress relief.
5)Low impact.
6) Resistance of water
")
")

")

")
")





")
")


")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
")
Benefit from Aqua therapy
- Reduce weight bearing on lower limb – helps in partial weight bearing walking gradation
- Assist in stability and balance
- Makes Movement easy and assisted
- Gives resistance to movements,
- Easy to change the grading of resistance
- High intensity training with less fatigue and injury to muscles and ligaments
- Less stress on ligaments in closed chain positions
- Helps in general body relaxation – stress management
- Joint mobilization hip, knee, ankle, shoulder & elbow with less pain even with high intensity mobilization
- Improving range of motion
- Spinal joint mobilization
- Muscle relaxation
- Non weight bearing wallking – deep water walking with floats
- Strength training
- Endurance training
- Agility & plyometrics training
- Balance training
- Reduce tone/spasticity /rigidity/ tightness
- Graded loading on labrum/ capsule and ligaments of joints
- Coordination training
Who can benefit from Aqua therapy
A. Normal population for fitness and aerobic conditioning, weight loss
B. Orthopedic conditions
1)OA knee
2)Arthroplasty ACL,MCL repairs
3)Knee ligament injuries – conservative/ post op
4)Rheumatoid arthritis/ Ankylosing spondylitis/ Poly arthritis
5)Spine – conservative/ post operative, Low back pain
6) Fractures – conservative/post-op
C. Neurological conditions
1. Stroke rehab, Hemiplegic- upper limb, lower limb and trunk control training, and strengthening, balance and gait training
2. Paraplegic and quadriplegic – upper limb, lower limb and trunk control training and strengthening, balance and gait training
3. Balance disorders, Parkinson, Ataxia – strengthening, coordination, balance and gait training
4. Peripheral nerve injury and polyneuropathy -strengthening and gait training
5. Traumatic brain injury
D. Pedriatics – Cerebral palsy, DMD, Spina bifida, ataxia, developmental delay -strengthening, coordination, balance and gait training
What are the contraindication?
 Frequently Asked questions about Aquatic therapy ?
Frequently Asked questions about Aquatic therapy ?
Q: Is it necessary to know how to swim for aquatic therapy?
A: It is not necessary to know how to swim, during therapy you will be supported by your therapist or floats.
Q: Can patients without bladder control/ with a catheter participate in aquatic therapy?
A: Patients without bladder control must empty their bladder before aquatic therapy session. In order to participate, patients using a catheter must obtain prior permission from their physician. During therapy, the catheter must be blocked. Due to risk of infection, some public pools might not permit patients with a catheter to enter the pool.
Q: Can patients with bedsore/ open wounds receive aquatic therapy?
A: Yes, patients with bedsore/ open wounds can participate in aquatic therapy after the application of a wet dressing (specialized dressing which prevents water going into the wound). Permission from your physician or surgeon is required before coming for therapy. Risk – there are chances of cross infection and delayed wound healing in some cases if proper precaution is not followed.
Q: Do I need to wear a swimming costume or can I come in regular shorts?
A: Everyone who enters the pool is required to wear a swimming costume. Men shorts and T shirt, Women can use short length or full body costumes. Women or men with long hair are required to wear swimming cap during pool sessions. (It is advised to cover body in order to prevent suntan)
Q: How many sessions do I need to take?
A: There is no right answer to this question. It depends on multiple factors such as type/stage/progression of disease, severity/level of injury, neuroplasticity and learning ability of patient, compliance to therapy, training intensity and frequency of therapy.
10- 15 sessions is recommended in order to evaluate the rate of change and the effect/intensity of therapy. Depending on the results, more sessions may be necessary.
Q: Will aquatic therapy benefit me?
A: Aquatic therapy is one of the modalities of physiotherapy, if you need/are referred to physiotherapy then aquatic therapy will be beneficial as well. Compared to physiotherapy on land, it is easier to move in the water and exercises in water are more fun. You will be assessed on land first to find your impairment, activity and participation restriction. Based on the assessment your therapist will decide if you need aquatic therapy or not. Most of the time a combination of land and aquatic based exercises are beneficial for patients for strengthening, postural/trunk control, balance and gait training.
Q: Can a patient with cardiovascular diseases have aquatic therapy?
A: Cardiovascular disease is not a contraindication but a precaution. Patients with poor cardiovascular capacity, lower ejection fraction, under active/unstable angina should not attend aquatic therapy. When a body is immersed in water changes in blood pressure occur, patients with unstable hypertension of hypotension should to be monitored.
Q: Will I be taught/allowed to do exercises on my own in the pool during/after my aquatic therapy session?
A: Yes, after receiving appropriate training from your aquatic therapist and you are safe to perform exercises by yourself. Make sure that a life guard is on duty and aware of you when exercising alone.
Q: How should I prepare myself for aquatic therapy?
A: Please note the following:
- Before aquatic therapy do not eat heavy food, light food or snacks are advised.
After a long session you might feel tired and hungry, therefore it is advised to bring a snack. - Keep well hydrated: Drink water before/during and after therapy.
- Empty bladder and bowel before therapy.
- Cover wounds with wet dressing before therapy.
- Take bath/shower before entering the pool.
- Check physical fitness and cardio vascular capacity, ability to tolerate exercises in water.
- It is advised to observe other patients’ treatment session to get an overall idea about the therapy in water.
- Bring moisturizer for use after pool session. Do not apply moisturizer before therapy otherwise it will be difficult for the therapist to maintain grip.
- Bring essential showering toiletries and a spare set of clothes (if necessary bring a person/aid for assistance before and after session).
Q: Are there any changes that need to be observed/reported after completing the session?
A: Please report the following after the session:
- How was the therapy experience?
- How did you feel during and post session?
- Did you notice any positive changes after the session?
For example: increased range of motion, strength, endurance, posture and movement - Did you notice any change in your functional ability, level of assistance or independence?
- Presence of any adverse reactions to water or worsening of your present symptoms?
- These issues may come up during the session as well, please report them to your therapist.
- Are you getting any muscle cramps or delayed onset of muscle soreness? If so, please report to your therapist. He/she will advise you on what to do about it.
Whom to contact for aquatic therapy?
Ans -Dr. Gajanan Bhalerao, 9822623701. schoolneurorehab@gmail.com
GB school of neuro rehab and aquatic therapy, Bungalow no 1. Gajanan Housing society Model colony Shivajinagar Pune 16. Direction and Maps










 4. These program are well organised and well conducted
4. These program are well organised and well conducted
{kind=link}
You must be logged in to post a comment.